By Karuna Jaggar, Former Executive Director and SABCS Guest Writer
 In our “take action,” “more is better,” “gotta do something” culture, most people assume that more medial testing will lead to better treatments. After all, many assume, the more we know about a specific cancer the better doctors can presumably tailor treatments. But the truth is many tests don’t make a difference for patient outcomes and sometimes medical tests harm more than help.
In our “take action,” “more is better,” “gotta do something” culture, most people assume that more medial testing will lead to better treatments. After all, many assume, the more we know about a specific cancer the better doctors can presumably tailor treatments. But the truth is many tests don’t make a difference for patient outcomes and sometimes medical tests harm more than help.
In fact, as we saw through several concrete and dramatic examples from this year’s San Antonio Breast Cancer Symposium (SABCS), some unhelpful tests lead to unnecessary and aggressive treatments. I found myself remembering the words of an internist I once had who said: “medical testing is like lint: it just keeps accumulating until suddenly you’re looking at a dust bunny in the room.”
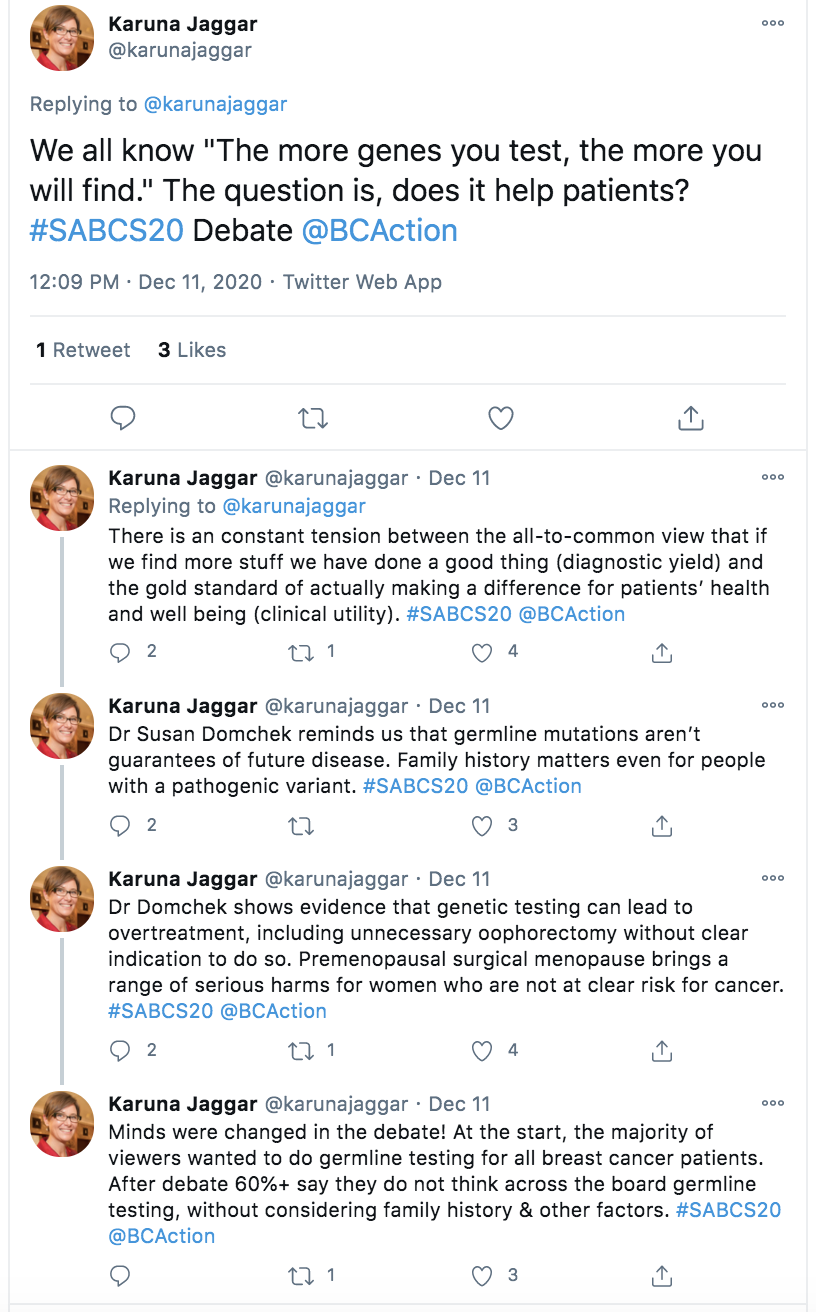
All too often, people confuse that diagnostic yield (finding more stuff) for clinical utility (making a positive difference for patients’ health and wellbeing). By keeping the focus on the gold standard of clinical utility—do patients live longer or fare better?—we can see there are, in fact, many reasons not to conduct some medical testing in certain situations.
The first standard of medical testing is simple: don’t do a test if it won’t change treatment. Other reasons include potential harms from testing that may outweigh potential benefits, such as adding to the cumulative lifetime radiation exposure or especially invasive procedures. Yet another important reason to avoid some medical tests is the likelihood that it may trigger a cascade of harms as a result. After all the Hippocratic Oath includes the promise “to first do no harm.”
Each year throughout SABCS I provide live commentary through Twitter, to both engage with other conference attendees and bring the lessons back to our broader community. Several of the topics touched on a common theme of when and why do perform a variety several common tests. Below are four Twitter threads as well as my synopsis of the relevant discussions.
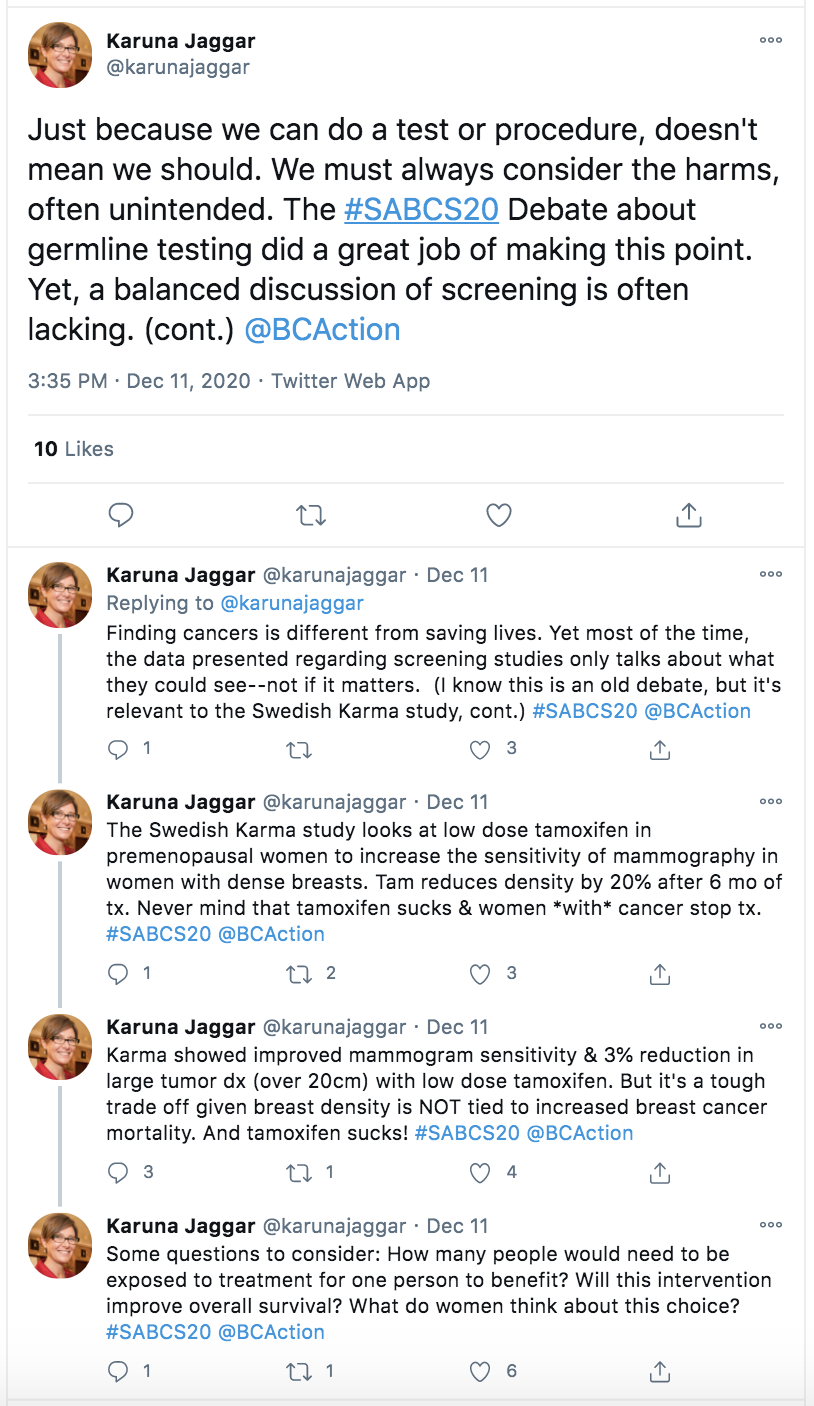
Breast cancer screening has become an area where it feels like the tail is wagging the dog. Rather than focusing on if and when screening reduces deaths, the unquestioned presumption is that the act of finding cancers is valuable in and of itself.
The Swedish team behind the KARMA study presented a poster titled, “Use of low-dose tamoxifen to increase screening sensitivity in mammography of premenopausal women” (PD11-07). They argue that “low-dose tamoxifen has the potential to increase the sensitivity of a screening mammogram and thereby reduce the proportion of interval and advanced cancers.” In other words, the researchers are suggesting that women take a low dose cancer drug (tamoxifen) in order to improve the detection of cancer, which will likely require taking that very drug.
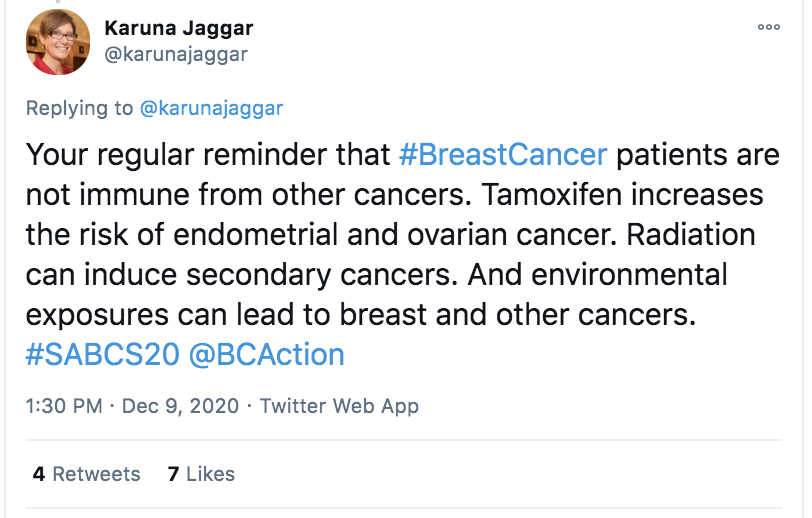
This isn’t even an argument for so-called chemoprevention (which Breast Cancer Action has written about extensively), but is an argument for what might be called chemodetection! And yet there’s no evidence that this will reduce death rates. Nor is there any acknowledgement that in addition to serious quality of life issues, tamoxifen increases the risk of endometrial and (surprisingly) ovarian cancers, as reported on Wednesday from the IBIS-II trial.
The Friday program included a debate on the topic: “All Breast Cancer Patients Should Have Germline Genetic Testing.” I was doubly interested, as the parent of a high-school debater and given my long-standing work on genetic testing.
The proposal was a scaled down version of Dr. Marie Claire King’s argument that all women age 30 and older should receive genetic testing, something which I’ve written about separately. This year’s SABCS debate featured Mark Robson, from Memorial Sloan Kettering Cancer Center, who argued for the proposal and Susan Domcheck, from the University of Pennsylvania, who argued against universal genetic testing for all women diagnosed with breast cancer.
Dr. Domchek dominated. She made a powerful case and convinced more members of the audience that widespread genetic testing can lead to overtreatment, including unnecessary oophorectomy and mastectomies, without clear indication to do so.
At the start, the majority of viewers wanted to do germline testing for all breast cancer patients. After debate 60%+ say they do not think across the board germline testing, without considering family history and other factors. It’s worth noting Dr. Domcheck’s expertise on the issue and her leadership as the Executive Director of the Basser Center for BRCA at the Abramson Cancer Center and the Director of the MacDonald Cancer Risk Evaluation Center.
Breast Cancer Action has written extensively about the complex issues surrounding a ductal carcinoma in situ (DCIS) diagnosis, which account for about 20% of all new breast cancer diagnoses, even though some experts argue that the word carcinoma should be removed from this non-invasive condition. Given my history of working on this issue, I was interested to learn—and share—the latest research from the Spotlight Session 5 on Thursday, “Current Concepts and Controversies in Ductal Carcinoma in Situ (DCIS).”
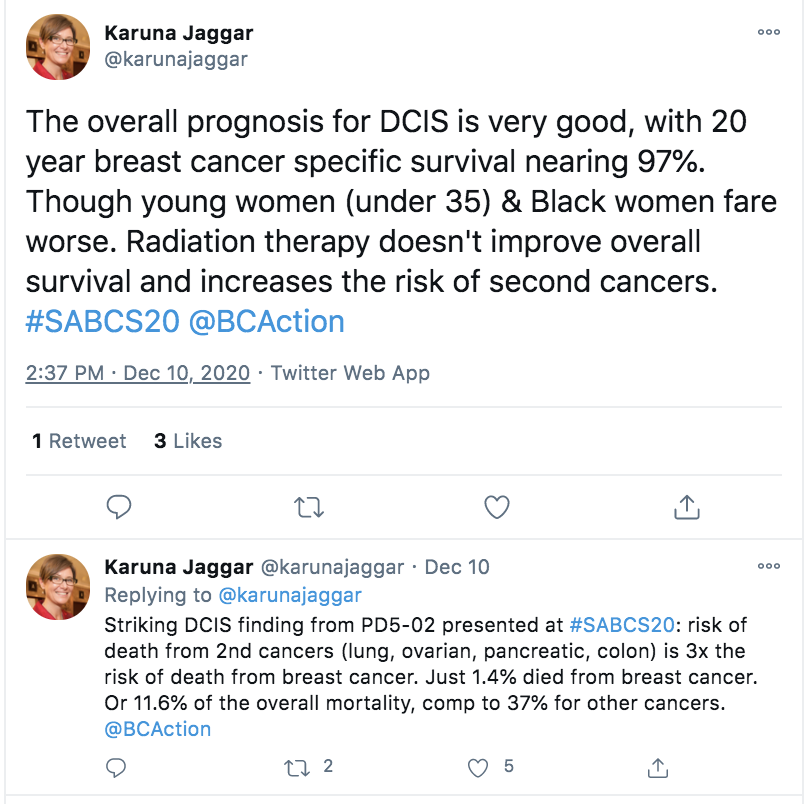
We have long known that the overall prognosis for DCIS is very good, with 20 year breast cancer specific survival nearing 97%. That’s remarkable and important to remember in any discussion about DCIS. Although it’s also important to recognize and account for the fact that very young women (under 35) and Black women who are diagnosed with DCIS fare worse, underscoring that there is no one-size-fits-all approach.
Although overall breast cancer mortality associated with DCIS remains very low, people diagnosed with the condition are at greater risk (some studies showing up to 30%) for developing an invasive cancer. Given the significant, often life-long harms of treatment, there are serious questions about if and how to treat DCIS, which many view as a risk factor for invasive cancer, rather than a “pre-cancer.”
For example, we know that radiation therapy doesn’t improve overall survival for DCIS yet it increases the risk of second cancers. Researchers found that the most common secondary malignancies from radiation include contralateral breast cancer (of the other breast), gastrointestinal cancers and gynecologic cancers. More recent cohorts also looked at secondary cancers for people treated for DCIS, and found that gynecologic cancers were the most common followed by lung cancer.
Breast Cancer Action has never pitted one cancer against another. And we’ve never been willing to trade one kind of cancer death for another. So it is more than sobering to recognize that the risk of death from second cancers (lung, ovarian, pancreatic, colon) is three times the risk of death from breast cancer after treatment for DCIS: just 1.4% died from breast cancer, which represents 11.6% of the overall mortality, compared to 37% for other cancers.
The harms and benefits of finding and treating DCIS are complex and require careful weighing.
The sentinel node biopsy technique, which lets surgeons evaluate the spread of cancer by taking just a few lymph nodes from the armpit, is one of the most important advances in reducing the harms of breast cancer surgery. Even though the technique was first developed and reported in the early 1990s, it has taken years to gain traction and it has not yet eliminated full node dissection, despite no overall survival benefit for taking all lymph nodes.
Even though it’s a smaller surgery, there are cases where even sentinel node biopsy is not necessary, including (as The Society of Surgical Oncology recommends) for women age seventy and older, with no clinical signs of spread to the lymph node. Yet eight in ten of these women get unneeded sentinel node biopsies. This is a powerful example of how difficult it is to stop doing a test once it has been introduced as standard of care, even if the evidence shows it’s not beneficial to patients.
Precision medicine is the idea that we might tailor treatment to a person’s specific cancer, if only we can understand the tumor’s molecular make up. The reality is we have a long way to go before such personalized treatments are effective—let alone affordable.
Despite the tendency to privilege biotechnological solutions to public health issues, sometimes low-tech public health measures produce more positive benefit. In 2018, Dr. Vinay Prasad published a paper in which he discussed with the ASCO Post where he shows that “the percentage of patients who benefit from genome-targeted therapy over time, it is about half-a-percent more patients per year.” The fact that approximately as many people will die of breast cancer this year as the year Breast Cancer Action was founded shows how far we still have to go to address and end this public health crisis and social justice scourge.
Looking at the lessons from this year’s SABCS, some of the key takeaways include: